

Abstract
Background:
Autologous stem cell transplantation (ASCT) is increasingly offered to older patients with multiple myeloma (MM) based on clinical trials demonstrating improved outcome. Inherently, successful mobilization and collection of peripheral blood stem cells (PBSC) is necessary for ASCT. A direct comparison of the efficacy of mobilization between elderly and younger patients has not been reported. Retrospective studies demonstrated that older patients had lower CD34+ cell yield and a higher incidence of mobilization failure (Lee et al 2014, Muchtar et al 2016). In this retrospective study, we compared two age groups (>/=70 years and <70 years) in MM patients who received ASCT at the John Theurer Cancer Center. We compared the outcomes of PBSC mobilization and transplantation between the two groups.
Methods:
MM patients who received a single ASCT at our institution between 2005 and 2016 were included. More than 95% of patients received either cyclophosphamide-based chemotherapy with GCSF (CY-GCSF) or plerixafor with GCSF (Pleri-GCSF) and were included in the analysis.
We identified 111 patients aged >/= 70 years and 315 patients <70 years. The total CD34+ cell yield, number of apheresis sessions and CD34+ yield per session were compared by age group and mobilization regimen using the student's t-test. Multivariate analysis was performed using the general linear model with age group, mobilization regimen, age and mobilization agent interaction, Durie-Salmon (DS) stage, disease status at mobilization, and mobilization within 12 months of diagnosis as covariates.
Progression-free survival (PFS) and overall survival (OS) were compared using Cox proportional hazard model with the above-mentioned covariates. All analyses were done using SAS 9.4.
Results:
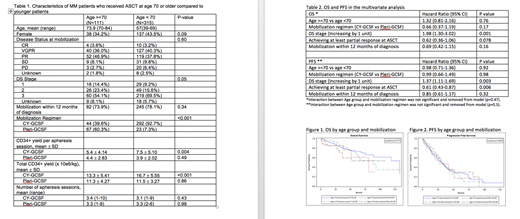
Patient characteristics and CD34+ cell yield by age group are summarized in Table 1.
The majority of patients in both groups underwent mobilization within one year of diagnosis. Older patients were less likely to receive CY-GCSF and more likely to receive Pleri-GCSF compared to younger patients (p<0.001). Disease status at mobilization, time from diagnosis to mobilization and DS stage were not associated with choice of mobilization regimens (p>0.05 for all).
The two groups had similar number of apheresis sessions regardless of mobilization regimen. When receiving Pleri-GCSF, the two age groups had similar CD34+ yield per apheresis (4.4x10e6 /kg and 3.9x10e6 /kg for age>/=70 and age<70, respectively, p=0.49). However when receiving CY-GCSF, the older patients had lower CD34+ yield per apheresis compared to the younger patients (5.4 x10e6 /kg and 7.5 x10e6 /kg, respectively, p=0.004). When comparing the CD34+ yield per session within the older cohort, the yields with CY-GCSF and Pleri-GCSF were similar (p=0.16).
In the multivariate analysis including all patients, time from diagnosis to mobilization, disease stage and disease status at mobilization were not associated with CD34+ yield per session or total CD34+ yield.
Neither age nor mobilization regimen was associated with PFS or OS, after adjusting for disease stage and disease status at ASCT (Table 2, Figure 1, Figure 2).
Conclusions:
CD34+ yield was comparable between younger patients and older patients receiving plerixafor + GCSF. In contrast, the CD34+ yield was lower in the older patients receiving cyclophosphamide + GCSF. The cause of the difference is not clear and warrants further study. The PFS and OS were comparable between the two groups after ASCT. The choice of mobilization regimen did not affect survival.
We have previously advocated cyclophosphamide mobilization in most patients because of the higher CD34+ yield and lower cost compared to plerixafor + GCSF (Panchal et al., ASH 2017). However this study showed that the CD34+ yield was not significantly different for patients aged 70 years or older in response to the different mobilization regimens. It is reasonable to consider plerixafor + GCSF in the elderly when chemotherapy toxicity is of concern.
Siegel:Karyopharm: Consultancy, Honoraria; Celgene: Consultancy, Honoraria, Research Funding, Speakers Bureau; Merck: Consultancy, Honoraria, Speakers Bureau; Janssen: Consultancy, Honoraria, Speakers Bureau; Amgen: Consultancy, Honoraria, Speakers Bureau; Novartis: Honoraria, Speakers Bureau; Takeda: Consultancy, Honoraria, Speakers Bureau; BMS: Consultancy, Honoraria, Speakers Bureau. Biran:Amgen: Consultancy, Speakers Bureau; Merck: Research Funding; Celgene: Consultancy, Honoraria, Speakers Bureau; BMS: Research Funding; Takeda: Consultancy, Speakers Bureau. Skarbnik:Gilead Sciences: Honoraria, Speakers Bureau; Abbvie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Genentech: Honoraria, Speakers Bureau; Pharmacyclics: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Jazz Pharmaceuticals: Honoraria, Speakers Bureau; Seattle Genetics: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Novartis: Honoraria, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal